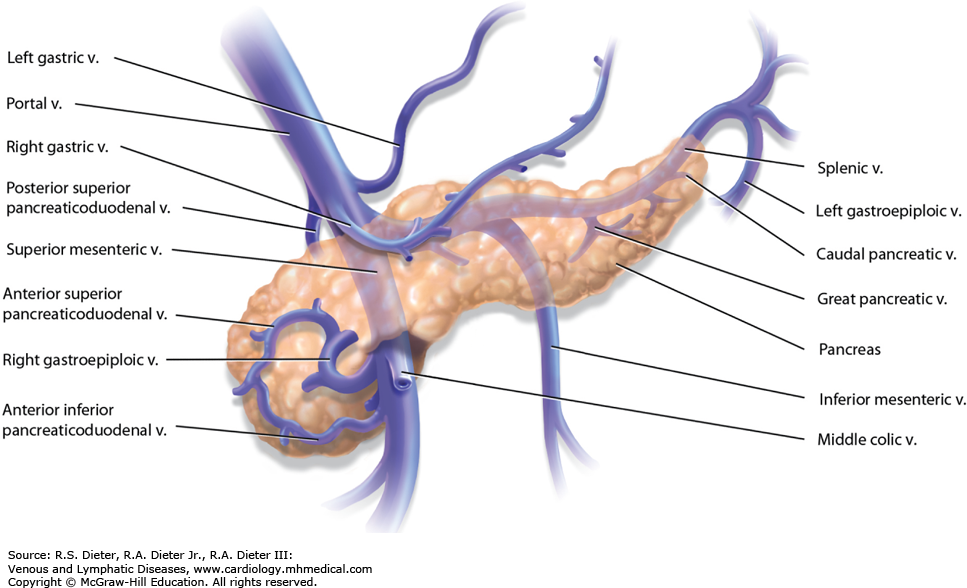
Q) Right gastroepiploic vein drains into
A. Splenic vein
B. Left gastric vein
C. Portal vein
D. Superior mesenteric vein
ANswer is free
MCH NEET SS Online Preparation
Q) Right gastroepiploic vein drains into
A. Splenic vein
B. Left gastric vein
C. Portal vein
D. Superior mesenteric vein
ANswer is free
Q) Malabsorbtive procedure in bariatric Surgery
a) Biliopancreatic division
b) Roux en Y Gastric bypass
c) Sleeve gastrectomy
d) LAp band
Q) Dumping all are true except
a) Conversion of BI to BII
b) More common in B1 as compared to BII
c) Most common after gastric pull up
d
Q ) Antral GIST 1cm incidentally found on UGIE. True regarding its management
a) Surgical resection resection of GIST (More questions on GIST here)
b) Endoscopic resection
c) Resection required if EUS suggests irregular border with cystic spaces
d) Endoscopic surveillance, if size >2cm then resect
Answer ( You need to be a premium member to see this)
GIST are usually found in the stomach (40% to 60%), small intestine (30%), and colon (15%). Clinically they appear in patients older than 50 years.
They generally have an equal male-to-female ratio or a slight male predominance.
They are rarely associated with familial syndromes such as GISTparaganglioma syndrome (Carney triad), neurofibromatosis 1, and von Hippel-Lindau disease, but most develop de novo.
Q) Gastric Lymphomas false is
a) The optimal treatment for lymphomas unresponsive to initial H. pylori antibiotic treatment remains unclear and includes the chemotherapy, radiotherapy, surgical resection, etc
b) Almost all MALT-lymphoma may regress with conventional H. pylori treatment.
c) Need for surgery in lymphoma is mainly for its complication
d) Risk of perforation is over estimated in the literature
Answer
Q) Antral GIST 1cm incidentally found on UGIE. True regarding its management
a) Surgical resection
b) Endoscopic resection
c) Resection required if EUS suggests irregular border with cystic spaces
d) Endoscopic surveillance, if size >2cm then resect
Ans
c
GIST more than 2 cm should undergo resection. Management of GIST less than 2 cm is dependent on weather high risk features are present on EUS.
The high risk features are
1. Irrgeular margins
2. Heterogenous architecture
3. Ulcers
Management of low risk GIST less than 2 cm is surveillance every 6 months
Q . Wrong about post gastrectomy syndromes (AIIMS MCQ 2018 GI)
A. Early dumping syndrome occurs after 1 hour
B. Early dumping syndrome has less cardiac and more gastrointestinal symptoms
C. Anastomotic ulcer is more after billroth II
D. Post gastrectomy syndromes are common in billroth II than roux en Y anastomosis
Q ) Hereditary diffuse Gastric carcinoma is associated with which breast cancer
A. Ductal carcinoma NOS subtype
B. Lobular carcinoma
C. DCIS
D. Metaplastic carcinoma
Answer for Q 79
Majority of Gastric Cancers are sporadic,
1–3% of GCs arise as a result of inherited cancer predisposition syndromes.
Li-Fraumeni syndrome, Lynch syndrome, Peutz-Jeghers syndrome, hereditary breast and ovarian cancer,1MUTYH-associated adenomatous polyposis (MAP), familial adenomatous polyposis, juvenile polyposis syndrome and PTENhamartoma tumour syndrome (Cowden syndrome).
Q) True about retained antrum syndrome after gastrectomy are all except? ( # MCQ in Stomach 11-15)
a) It is a persistent hypergastrinemic state
b) It is only seen after Billroth II Gastrectomy
c) Technetium labelled food is not helpful in diagnosing this condition
d) Serum gastrin is usually less than 1000 pg/ml
Answer c
After billroth II gastrectomy, if a cuff of gastric mucosa remains with duodenum, this entity is called as retained antrum syndrome. This cuff of gastric mucosa is cut off from the proximal stomach and inhibitory effect of hormones such as VIP (Vasoactive Intestinal Peptide) leading to a persistent hypergastrinemic state. ALso this gastric mucosa is continuously bathed by the alkaline contents of duodenum , which further increases the acid formation.
Both Basal and maximal gastric acid outputs increase but it is not as high as seen in zollinger ellison syndrome. Typically less than 1000 pg/ml
This condition can present as recurrent and persistent ulcerations. Technetium scanning is the diagnostic modality of choice. Treatment is re do surgery and antral excision.
Technetium pertechnate imaging has a sensitivity of 73% and specificity of 100%
Diuelafoy lesion which is false? (AIIMS 2018)
A. Most of the bleed cannot be visualised due to small mucosal defect lies over large arterial
bleed.
B. Large 1-3 mm artery in the submucosa is the source
C. MC in the greater curvature
D. Found within 6 cm from GEJ